“Strawberry Milkshake Blood”: A Real Lab Story About Lipemia and Why Med Tech Judgment Matters
This is a real case of “strawberry milkshake blood” (lipemia) and how experience prevented a false critical lab result.
Most patients never see their blood after it leaves their arm. They see the needle, and later they see numbers in a report. But in the clinical laboratory, we see what happens in between, and sometimes there are little dramas.
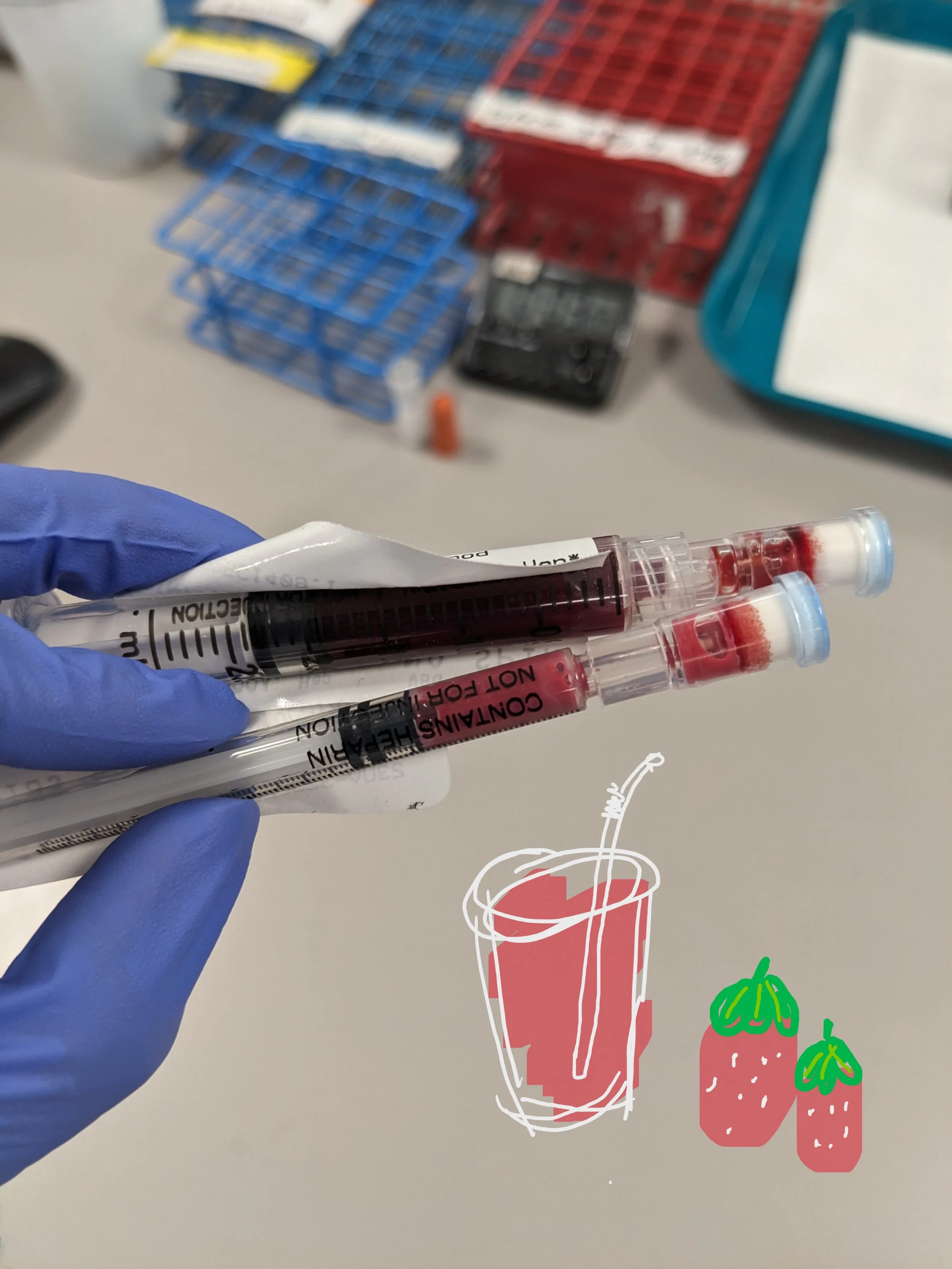
One time, I received a blood sample for a blood gas test that immediately caught my attention. The blood looked pink; the plasma looked creamy after centrifugation. This is a textbook classic “strawberry milkshake blood.” The technical term is lipemia, which usually refers to the bloodstream containing extremely high levels of fat particles, particularly triglycerides.
We ran the blood gas. Everything is in the reference range. A few minutes later, another sample arrived from the same patient, ordered for a Basic Metabolic Panel (BMP). When the results appeared, something odd happened: the CO₂ value came back critically low.
The standard protocol is to call the floor to report a critical result. But something didn’t feel right.
The blood gas from just minutes earlier showed no abnormal findings. I checked the patient’s chart and found no alarming vital signs or notes that could be related to primary metabolic acidosis. After working in the lab for years, you develop a sense for when a result doesn’t quite match the clinical picture. So, instead of calling the critical result immediately, I decided to do a quick little experiment: I performed a superspin, a high-speed centrifugation used to further separate lipids from plasma, and reran the tests: aha, the critical value disappeared.
Our chemistry analyzer uses reagent coated dry slides for all tests in the BMP, and the result readings are based on color changes on the slides. Usually, lipemia doesn’t cause major problems with this method because turbidity has such a minimal impact compared with liquid assays, so the standard procedures don't put the sample through a superspin for the slide assays. However, this sample was unusually lipemic, sooo lipemic that the result is interfered.
I contacted our on-call resident to explain the situation, and the case was escalated to the medical director. The final decision was to release the value from the superspun sample, off procedure. One likely explanation was that the "whiteness" of the lipid particles partially masked the color change used to measure CO₂, producing a false critical result; the other possibility is that the volume displacement is so large that the aqueous phase where it is measured is simply reduced too much; or maybe both conditions contributed to the false alarm together.
Cases like this remind me why clinical laboratory work is more than simply releasing whatever number the analyzer produces, even you have 100% followed the verified instructions step by step. Machines are powerful tools, but they don’t understand context. Experienced laboratory professionals can recognize when something doesn’t make sense. If I had called that critical result immediately, no one would have blamed me, but taking an extra moment to think about the result ensured the patient’s report was accurate and maybe even prevented harmful treatments.
Sometimes, behind a strange looking tube of blood, something that resembles a delicious strawberry milkshake is a reminder that laboratory medicine still depends on human judgment.